

NSW Clinical Excellence Commission’s new Environmental Cleaning Audit Tool
by Ellen Hingston, Environmental Services Manager, HealthShare NSW
At our recent Hospitality in Healthcare industry breakfast session held in Sydney, HealthShare NSW Environmental Services Support Manager Ellen Hingston gave a presentation about the new Clinical Excellence Commission’s Environmental Cleaning Audit Tool. The tool went live last month and its use will become mandatory across NSW Health facilities later this year to support a consistent and standardised auditing approach.
For the benefit of those members who couldn’t attend the Sydney briefing, Ellen has provided the following article explaining the rationale behind the new Audit Tool and what it entails.
Why do we need to conduct audits?
Cleanliness in healthcare facilities is mandated by the Cleaning of the Healthcare Environment policy and is considered a key part of the infection prevention and control program in NSW Health.
Maintaining high standards of environmental cleanliness isn’t just about infection prevention and control. It also contributes to work health and safety; comfort and wellbeing; protecting and prolonging the lives of our assets; maintaining the reputation of the facility; and supporting public confidence.
Auditing of environmental cleaning means checking that the cleaning is done to a high standard, using a systematic, independent and documented process, and providing feedback.
These audits help identify risks and inefficiencies, promote compliance and improve overall effectiveness, productivity and staff satisfaction. Audit reports also provide evidence of compliance for accreditation and inspections and when responding to complaints or claims.
Key requirements of an audit
The Cleaning of the Healthcare Environment policy outlines clear guidance on conducting audits:
All NSW Health organisations must have a cleaning audit system that measures and records cleaning outcomes.
Cleaning audits must be performed in all functional areas across all risk categories.
Health workers undertaking audits must be trained and have thorough knowledge of cleaning standards and processes.
Where possible the auditor should be accompanied by a staff member from the area being audited.
Where compliance is not met, action plans are implemented within set timeframes.
Results, plans and outcomes are to be documented and reported to appropriate clinical governance committees.
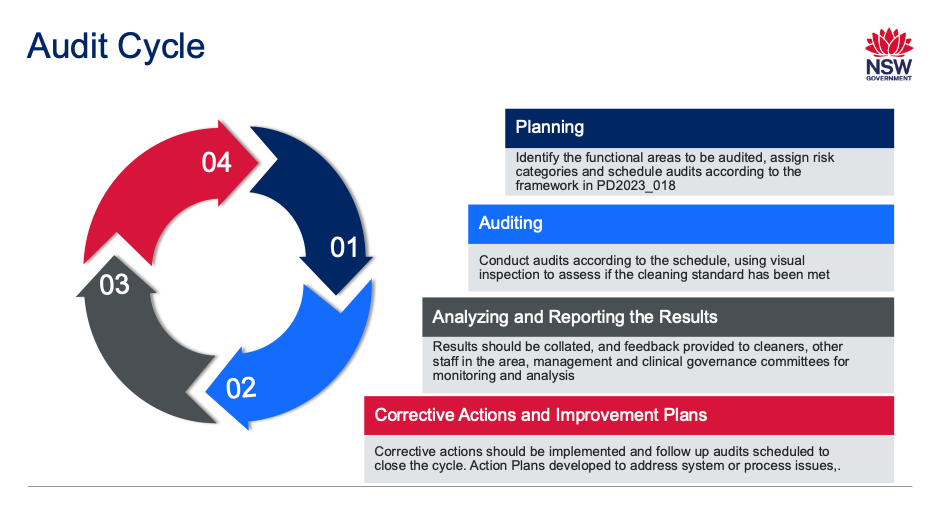
Step 1 – develop a plan and schedule audits
The first step is to identify the functional areas, usually a ward or department, and assign a risk category based on the risk and likelihood of negative events associated with cleaning.
A schedule should be developed to ensure that the audits are conducted according to the frequency specified in the policy and that resources can be allocated.
Step 2 – visually inspect the area and documentation
A person trained in auditing undertakes a visual inspection of an area and documents the inspection.
Frequently touched surfaces in patient care areas should be cleaned more often due to an increased risk of contamination, and auditing should reflect that. However, all surfaces should be included in the environmental cleaning audits, including those that are inaccessible.
Each question is scored and an overall score for the functional area is obtained.
Step 3 – analyse and report
Results of individual environmental cleaning audits should always be fed back to cleaning staff and management, as well as Infection Prevention and Control (IPAC) and other department staff members, to support a local culture of accountability and increase knowledge about environmental cleaning.
Environmental cleaning audit results should be stored centrally and results, trends and issues regularly reviewed and discussed at the relevant governance and/or organisational committee meetings – eg Infection Prevention and Control (IPAC) or Clinical Governance.

Step 4 – develop corrective action plans
Cleaners and management, in consultation with ward staff, department heads and IPAC should develop and implement Corrective Action Plans to rectify immediate issues identified within the required timeframes and address gaps or system issues that may be barriers to effective cleaning.
In real life situations steps 3 and 4 will often overlap and be completed simultaneously. A complex Action Plan to address a systemic issue will likely take more than one audit cycle to complete.
Why we needed a new Audit Tool
The first Clinical Excellence Commission (CEC) Audit Tool was developed alongside the first Environmental Cleaning Policy in 2012 but while the audit frequencies and required standards were mandated, the use of the CEC tool was optional.
To achieve a more consistent approach, the CEC and the Environmental Cleaning Advisory Committee, which includes representatives from local health districts and other health organisations, have been jointly working on a new Audit Tool to:
develop a simpler tool with less questions and better flow
ensure the questions are clear and that every area within the location is covered by a question
increase focus on the patient environment
facilitate benchmarking between facilities by standardising the tool and making it mandatory.
Using the Audit Tool
The Audit Tool has been designed to assist and guide in inspecting how well the various functional areas and the elements in those areas are cleaned.
Most of the questions are in the Yes/No/Not Applicable format. The minimum required standard is ‘visibly clean’ which means free from dust, soil, mould, stains, smudges, cobwebs, body fluids, and soap, mineral or chemical build up.
Any question which is relevant to the area being audited should be marked Not Applicable, those questions do not then contribute to the final score.
The questions have space allocated for comments, which can be used to clarify or identify specific areas of concern. Photos can also be attached to the questions to illustrate the problem or to show a specific location. Using comments and photos assists with identifying rectification cleaning that is required and supports preparation of plans to improve cleaning outcomes.
The tool is now live and feedback can be provided to the CEC up until 1 June 2026 using CEC-HAI-IPAC@health.nsw.gov.au. Those responsible for auditing of environmental cleaning in NSW Health facilities should take this opportunity to trial the new tool and to provide feedback.
Following the pilot period, the finalised Audit Tool will become mandatory for all NSW Health Facilities to meet the auditing requirements of Policy Directive Cleaning of the Healthcare Environment later in 2026.